Welcome to WordPress. This is your first post. Edit or delete it, then start writing!
Category: Uncategorized
-
The Blog Rounds goes summer experience hopping!
 Summer fun?
Summer fun?Check out what MDs do come summer time! Watch out for the upcoming fifth edition of The Blog Rounds, themed “I Know What You Did Last Summer!” to be chronicled by Doc Ness in her blog, At Random Ness!
Deadline for submission of blog entries will be on April 15, 2008! Guidelines for submission can be read here. Visit Doc Ness blog for the edition’s theme and additional guidelines.
-
Our marvel of a survivor!
“What??!!” was my bewildered reply to the nervous voice on the phone line. I stood silent for a minute, holding tightly to the phone on my ears and staring blankly on the corridors of ward 8. Feeling the cold sweat engulfing my consciousness, the world around me suddenly turning into a gyroscope of blurred images. The universe went dark.
“Doc? okey ka lang?” came the ward nurse’s faint voice. “I need you to sign this” handing me a patient chart needing an RIC’s signature. I cleared my throat and mustered enough energy to sign the chart with my hands shaking. “Sigurado ka okey ka lang doc?” She asked again. “Thank you” I said, motioning her to go away and making a gesture I’m answering a call.
I haven’t turned off the phone yet.
I’m seeing her face- short, gray hair that was always kept tidy by constant rearrangements. Her cheerful face look a bit weathered but is still wittingly sharp, beaconing years of endless struggle to survive a harsh, defiant world. Lately, wrinkles appeared in her forehead and no matter how she ‘tucked” those with make up, age seem to catch up with her indomitable spirit.She use to wake me up in the morning with “kain na!!!!“and then bang my door.
She was just fifty and I just finished med school.
“She went into the provincial hospital without informing anyone about it. Not even us. I only found out when she called after the operation.” My sister’s nervous voice collapsed into sobs of frustration. Dumbfounded of the events unfolding, I can neither summon enough energy to console my sister nor think clearly about the situation we were in. It was a chaotic tug of war between uncertainty and frustration. I am totally dazed.The mixed emotions of grief, fear, anger and love, all bursting up front.
What if we lost her? Are we prepared for this? Is she prepared for this? I shiver at these possibilities.
A marvel of parental control and survivorship, she lost her husband while in her early forties. She took the cudgels of single handedly supporting their four children, sending them to through college and produced four top caliber professionals in their fields. For the longest time she was the family’s beacon, the passion, the inspiration. And now the danger of suddenly “losing her” lurks just around the corner.
She is Helen.
Helen is my mom.
“Well differentiated uterine adenocarcinoma,” came the histopath. Silent panic. The sudden gush of adrenaline made my heart thump louder I could hear them between my breaths. The phone almost slipped my hands while I froze in disbelief. Now, losing my mom is a grim possibility. What now?What shall I do? What shall we do? Med school had trained me for situations like this. But not if your mom (or any other close person) is the patient.
Med school even made it more painful for us doctors. We often have an idea how disease progress and how it eventually ends.
“Sir can I file a leave starting tomorrow?” I told my team captain and chief resident. “My mom have uterine CA and will undergo surgery in our province“. My chief resident looked at me for a while and sensing some desperation said “Ok. You can file your leave and go home a soon as you endorsed all your patients. But come back !” He too can sense the frustration and hopelessness in me.
Yes sir” I subconsciously answered . I was busy thinking about my mom.
I’m still lost in “what ifs”
Arriving early in the airport next day, I went directly to the hospital and into my mom’s room. Asleep with IV lines jutting out of her forearm she looked pale from the blood loss of prolonged menstrual bleeding before. She is cachectic and visibly weakened . “She lost this much…” I whispered. I looked at her teary eyed. I wanted to hug her tightly, but never had the courage to do so. Her sunken, gray rimmed eyes suddenly opened. She was surprised to see me there and hugging her. My mom is not used to this hugging thing and she hates being pitied upon. “Bakit?” was all she said. I didn’t answer. I just sat in the chair beside her bed.
“We’d be doing a Total Hysterectomy tomorrow. She won’t need her ovaries too so we’d take it as well. Problem is she has diabetes.” Her OB Gyn told me. “Diabetes???” I remembered my mom siblings got diabetes too, so it is really possible my mom has diabetes but she was mum about it. My heart melt in pity for my mom. She couldn’t just take all these diseases in one single hospitalization! If she is lucky enough to survive the CA, she has to contend with another equally debilitating chronic disease!
After all she had done for us?? This is all she will get??! It’s not only unfair but entirely painful!
I sprang into a robotic action, called all the MDs I know, asked for advices and called a family meeting. That family meeting seem like eternity. I could feel the tons of weight that stood on our shoulders. “I am the doc and I know what to do.” That’s what is expected of me and that what I’m hypnotizing myself with. Hopefully it will work out.
My brother and sisters all waited silently, visibly grief- stricken. We abruptly “lost” our dad before too. Such sudden turn of events not only traumatized our poor souls but made us grappling for lifelines too. The fact that none of them has had any medical background added more to their uncertainty. The burden is so heavy. “You decide because you are the doctor and you know what to do” said our eldest. I always dread this phrase. It makes me feel like dying too.
“We will all suffer and grieve, If we will all just cry here and do nothing ” I said in a crackling obviously pretending voice. But we’re ready to strike a deal with fate just to extend my mom’s life. She was our lifeline.
Hiding the panic in me, I went organizing a support group for my mom. “We have to adapt to the current situation or we will suffer. “ I made roles and schedules for each of my siblings- preparing food, relieving hospital watch, even informing contacts. I was busy arranging for the OR, finding the necessary meds, medical needs and preparations. I pretended to be the “in charge guy” but deep inside I’m cracking up in panic and fear.
“I’ll advised” said my friend.
I decided to scrubbed in the OR next day. My mom’s surgeons let me in and used my “surgical” hands too. It was an all star surgery for a routine hysterectomy. An OB gyne doing the surgery, a general surgeon assisting and an orthopod on the second assist and another MD on third assist. We have an internist watching over my moms medical condition the whole OR There two anesthesiologist working behind the bags and machines. Outside the operating theater were hordes of close friends watching the show.
I don’t know, but whenever I went into the surgical room, my panic temporarily stops. I feel as cold as any steel as the scalpel I’m holding, perhaps a result of years of training. The team went into robotic precision the entire surgery. I distracted myself not to think about the patient on the OR table, so I don’t clutter or be jerky assisting. The surgeons were meticulously well oiled and systematic. After swiftly removing the uterine and ovaries, we inspected all the nodes and noted for gross metastases. We did the routine inspection three times. None were suspicious. My mom’s appendix is “inflamed” so the surgeon removed it also. I was totally engrossed in the procedure I didn’t notice we were already an hour into the surgery. “Wash!” Woke me up and made me realized the surgery will soon end. After final last minute check of organs, bowels, instruments and sponges, we closed the incision. It was an uneventful procedure and we were all happy the team is through these emotion filled surgery. I made a little speech to the OR team thanking them for helping my family all out and making this surgery safe and succesfull for my mom. I was surprised by the round of applause the team gave each other.
Two days after, my mom was already walking and taking her bath alone. She was visibly rejuvenated but is still weak to walk unassisted. Her blood sugar stabilized and she was eating quite well. There is this smile on her face already. My pamangkins were all around her playfully tagging their lola. Helen is all smiles facing and talking to all those visitors she had like nothing happened.
We were happy too. She went to live another lifetime we believed. Perhaps several years more who knows. For once we were suddenly reminded of our moms loving presence. That in the process of us growing, we never had noticed she was getting old also. And as me and my siblings looked at each other, we knew right then we’d be better off showering our mom with love or we won’t have time for that at all!
The tumor margins were negative for mets. The review of slides were the same adeno CA initially diagnosed in our provincial. I brought my mom to a well known gyne-oncologist in Manila for another follow up check up. He said that my mom luckily survived the ordeal. He advised yearly abdominal CT Scan. For 8 years now, my mom has been symptom free. She had her swings of glucose intolerance but this can be adequately controlled medically.
She still hates being pitied upon or being thought of as weak. If my dad “thought” of everything he wanted us to become, my mom carried the four of us to an unbelievable life struggle, never hinting for moment about quitting or saying “I can’t”.
My mom is a marvel of a survivor.
-
At A Crossroad: The Blog Rounds 3rd ed is up at In the Middle of Nowhere
(The original picture in this post is owned by Kenny Gulley, entitled The Storms of Life, was removed upon the owners request, depicts a man at a “crossroad”)The thousands crossroads we face in our daily lives. Who makes these crossroads? Who serves us the options? Why do we have to face it? What makes us choose the road less traveled? How do we feel about our decisions now? Are we happy about it?
These are some of the questions physicians have dissected, researched and the answers, blogged in The Blog Rounds 3rd ed. Themed “At a crossroad“, the third edition of The Blog Rounds is up at Doc Claire‘s blog In the Middle of Nowhere. In this edition, you will see a growing community of Filipino doctors who blogged about their personal and medical life! What they wrote, will actually fill my whole week of reading and pondering!I am very thankful Doc Claire accepted and run a well thought of third edition of TBR. I am very much excited also of the growing number of Filipino MD blogger who joined TBR! My hat’s off to all of you!The Blog Rounds is a weekly compilation of the best in Philippine’s medical blogosphere, written by physician bloggers (or the medically inclined bloggers) and hosted on a participating blogger’s weblog. Archives and edition schedules ( plus the host blogger) are listed here. The next edition of TBR will be up this Tuesday, April 8,2008 7am PST and will be hosted by Doc Tess of An Eye Doctor in a Third World Country. For physicians and medically inclined bloggers interested in joining this blog carnival, please contact me through my email kokegulper[at]yahoo[dot]com or any of the participating TBR bloggers. Guidelines and updates are posted here in my website, The Orthopedic Logbook. -
No where to go but up!
(I wrote this article while savoring the brutality of starting a practice and endless whining of a slow start.)
My struggle has always been between filling up my empty stomach or satisfying my impoverished brain. To the millions of hungry Filipinos like me, this our “class struggle”-an unarmed, non-violent but similarly aggressive perspective of seeing past our choices of everyday life.
To a proletarian who have gone to the bottom lowest of the pits, the best assurance one can get whenever you start a career or something is an old adage that says “you can go nowhere but up” or something to that effect. Like a messianic prophecy, I fanatically held on to this belief since high school days . The capitalist notion of incentive-driven success vis a vis hard work is as ironic as it is baffling to everyone in this “stomach” struggle. Yet, I survived half of my lifetime living in such altruistic ironies that neither my myopic deconstruction of choices nor the risky jumps I made could explain the extraordinary luck I had ending up being a physician.
The dream of donning a white blazer and treating a patient is as fascinating as it is exciting. I am so entwined with that dream I forgot I have neither the financial capabilities nor the intellectual giftedness needed to attain such lofty dreams. I went into this profession simply because I wanted to prove to myself (and to my less encouraging social caste) what everyone in my bunghole has failed to do before me- don the white blazer with the least expense I can- financially and intellectually that is. Everyone think it was suicide in the making. I thought I have nothing to loose. I don’t have anything to loose anyway.
That dream however grew into a vision, thanks to my alma mater. I practically crawled and bled to finish top of the line education for a career not everyone in my caste will experience- not even in their dreams. Fifteen years of Hippocratic studying did wizen my outlook about this noble profession. But it also shattered some idyllic notions I once have about doctors’ blissful life. More importantly, it brought my bourgeois upbringing to its knees and gave me the awakening of my comfortable life. My mission is never confined to the personal and financial self gratification kind of success. Because if it is that myopic, I could have never gotten this far.I have all the necessary ingredients for a successful medical practice. Ingredients that when “cooked” rightfully, would lead me into the much coveted goal in life that is termed success. Such “ingredients” are big words indeed, taught in bold letters, eaten in gastronomic amounts and digested in herculean way. It’s funny after that word found its way into the neurons of my brain, I have been deluded of a blissful life outside the academe, akin to the Renaissance Man. Little did I know about the truth that lay ahead in real medical life that is called “the Practice“
Starting an upstream professional career is never an easy thing for the not so typical surgeon wannabe like me. I neither possess the inherited practice most other surgeons nor the coffers to buy a new one. Most people believe though, that having trained in one of the best medical schools in the country prepared me for one of the most formidable foe of the real life physician practice- an empty stomach.Of course being out of the academe and starting your own practice has its exciting advantages. The thought of having to take control of one’s time and spend it according to what you want is exhilarating. I can spend more time with what I want most, or with my loved ones I neglected when I was still studying. Gone are the Sundays where you have to read and prepare for pre-ops instead of having to eat dinner with family. I see non emergency patients on a scheduled time I myself created. Most of all, I have time to take care of my body while taking care of patients as well. I can eat full meals in a day and exercise regularly to maintain a sound and fit body. It is ironic that while we take care of patients 24/7 in a hospital, I lost tract of my own health in the process.
I am into the practice of my profession for just barely two months, and it’s neither the blissful stride I once dreamed nor the catastrophic frustration I’m so afraid of before. Somewhere in between these extremes is the horrible spectrum of uncertainty where my minute practice existence resides. I wish my practice was as dramatic as the scenes in ER and Grey’s Anatomy or as wacky as unnerving as House’s one liner ass kicking. Nonetheless, the uncertainty gave me ample excuse to whine and be cynical about everything I get my hands on. Blame it on inexperience surgeon wannabe that is me. Everyone says that staring a career is shitty enough to make or break your soul. My soul has undergone so many breaks it neither can feel any shattering this practice has to offer nor enough time to recover form constant battery of changing lucks past choices.
I bet it’s easier to just look at it as the paradigms of opposites. The definitions of success (and failure) in ones’ professional practice defined by simplistic phrases like-great clinic practice, successful surgeries, acknowledged researches, magnanimous services to patients and yes, professional fees enough to buy what we need. In essence, the very opposite of such adjectives and superlatives defines failure . Of course almost everyone believes that such simple dichotomous definitions don’t exist in reality. The theory of relativity seems to apply even in the psychology of success.
So it seems. But that, I have yet to uncover.
(Photo credits: All photos were taken from Deviant ART, my favorite repository of artistic shots.)
-
Call for articles and updates on The Blog Rounds
Even the real edema rounds “rest” during holy week! So is The Blog Rounds! But now that the Lenten- blogging holiday is over, TBR will resume making rounds!

The Third edition of TBR will be hosted by Doc Claire‘s Chronicles from the Middle of Nowhere. Call for articles and entries is up here. Please visit Doc Claire’s blog for the edition’s theme and additional guidelines.I’d like to congratulate Prudence MD (for hosting TBR) and the blogger contributors ( Doc Tes, Doc Ness, Pinay Megamom, Joey MD) for the very interesting Second Ed of TBR. We’re glad Pinay Megamom and Joey MD joined TBR already. Doc Tess and Doc Ness, saludo ako sa inyo! You both blog ala naturelle!
For those unaware yet, The Blog Rounds is a weekly compilation of the best in Philippine’s medical blogosphere, written by physician bloggers (or the medically inclined bloggers) and hosted on a participating blogger’s weblog. Archives and edition schedules ( plus the host blogger) are listed here. The next edition of TBR will be up this Tuesday, April 1,2008 7am PST.
Physicians and medically inclined bloggers interested in joining this blog carnival, please contact me through my email kokegulper[at]yahoo[dot]com or any of the participating TBR bloggers. Guidelines and updates are posted here in my website, The Orthopedic Logbook.
-
The Orthopedic Logbook on Physical Fitness and Conditioning for Mountaineers
 The author with a few trekking pilgrims to Mt. Apo, post for a group picture while at camp at the highlands of Makalangit, New Israel. This camp is considered station 10 of the long, arduous station of the cross climb towards Mt. Zion-just north of Mt. Apo
The author with a few trekking pilgrims to Mt. Apo, post for a group picture while at camp at the highlands of Makalangit, New Israel. This camp is considered station 10 of the long, arduous station of the cross climb towards Mt. Zion-just north of Mt. ApoThe “holy week” is of special interest to outdoor pilgrims like me not only because of an important Christian tradition it celebrates, but also because of the long vacation time it offers. It give us trekking saints longer time to troop to our mecca hit those peaks again! I am one of those outdoor buffs who spent the last two successive Lenten season on top of those mountain ranges.
Ironically, no matter how low profile I keep on what my real job is, I often get questions related to it and mountaineering, a hobby I soon enjoyed.“How do you physically prepare for this climb Dokie? Is there a way for us to prevent injuries and muscle soreness during and after climbs? Why do some people pass out of exhaustion or get headaches at high altitudes?”
These are the common questions fired at me, by my climbing buddies and often by newfound trekking friends.
 Oftentimes asked about questions related to his job and his hobby, like in this picture, a post climb socials, the author sometimes grapples for answers he wished taught in med school and training.
Oftentimes asked about questions related to his job and his hobby, like in this picture, a post climb socials, the author sometimes grapples for answers he wished taught in med school and training.Sometimes, I wish I have a tape player with me, so I could replay my answers to these questions. Because of these recurring questions, I have been inkling to write about the medical aspects of mountaineering. Specifically, I would like to start off with physical fitness and conditioning based on what I know and experienced, both as an orthopedic surgeon and an aspiring mountaineer.
 The author after a extremely cold night on top of Mt. Dulang-Dulang, in a recently concluded double major, double strenuous traverse climb
The author after a extremely cold night on top of Mt. Dulang-Dulang, in a recently concluded double major, double strenuous traverse climbA word of caution though. As much as I want to claim bragging rights of being a mountaineer, I am still a novice in this sport. That I am an expert sport physician and wilderness doctor is also too capricious a title. But I have developed a fitness program for myself, trekked a few mountains (read my other blog, Talakudong Mountaineer), endured some accidents and injuries from climbing but was able to go back to work as an orthopedic surgeon again. That in itself perhaps led me to study and learn more from my experiences and share it with anyone willing to learn and try it themselves.
 The author, after a river trekking (Penek Busay, Digos) accident last September 2007, sustaining bilateral 2 inches gaping cut on both his knees.
The author, after a river trekking (Penek Busay, Digos) accident last September 2007, sustaining bilateral 2 inches gaping cut on both his knees.Physical fitness and conditioning for mountaineering is a complex topic to discuss, often involving the ideas of a multi specialty training team but basically anchored on sound scientific, medical principles that is fine tuned by personal experiences. My fitness regimen was a product of reading, experiences of me and others I know, of trial and errors, of accidents and injuries I got whenever I hit the peaks or outdoors. I realized though that such experience and knowhow is of no use if not shared or taught to newbies willing to learn, and to experienced climbers avoiding accidents to happen while at their beloved sport.
Before we go further, I highly recommend that any serious climber should seek advise from their physicians before embarking on this task or scaling any mountains. In developing a fitness training program for your mountaineering expeditions, I also suggest the guidance of a certified fitness instructor. I understand that these two person may not be available in certain areas for certain people either for monetary reasons or lack of specifically trained personnel. But these are essential persons if you want to have a fun and less strenuous, less accident prone climbs. There’s no doubt about that. Ultimately, I (and this blog) hold no responsibility for whatever will happen to you, on training and on your climbs, whether you’ll follow my advise or not. That is entirely a personal
risk you have to take.Personally, I always make it a point to know my current fitness status and goals before I embark on a training program or climb. There are numerous factors that can affect the fitness capacity of any person scaling a mountain, be it the weather, difficult trails, steep inclines and the altitude itself to name a few. To be able to face these unforeseen factors squarely and hurdle them, you have to be fit enough to adapt and survive. Aside from your basic mountaineering skills and survival tactics, this is where a fitness program and physical conditioning is all too important and beneficial.
 Chris and Lemuel, the author’s climbing buddies while maneuvering a 20 meters slippery 90 degrees steep descent, holding only to jutting root parts and mostly dangling helplessly with no footholds. This is an extreme, “hard core” trail we manage to pass during our late traverse climb in Bukidnon.
Chris and Lemuel, the author’s climbing buddies while maneuvering a 20 meters slippery 90 degrees steep descent, holding only to jutting root parts and mostly dangling helplessly with no footholds. This is an extreme, “hard core” trail we manage to pass during our late traverse climb in Bukidnon.A good fitness program for mountaineers consist of two major groups of exercises, the cardiovascular (aerobic) and motor (anaerobic) fitness exercises. Cardiovascular fitness is measured by your aerobic capacity to take in and use oxygen. In most instances, this is a function of pumping blood (and oxygen) into the muscle system with the help of lungs. A motor fitness program consists of exercises to enhance strength, endurance, power, balance, agility and flexibility. With better cardiovascular capacity and good motor fitness, the third component of fitness training for climbing, which is acclimatization, will be a little less painstaking.
 The author, on top of one of Mt. Apo’s peaks, terribly out of shape but happy. He promised to develop a better physical fitness and conditioning for himself next climb. (Aguilar 2007)
The author, on top of one of Mt. Apo’s peaks, terribly out of shape but happy. He promised to develop a better physical fitness and conditioning for himself next climb. (Aguilar 2007)For purposes of discussion, I’d be using the goals I set for climbing Mt. Apo (which I climbed on a Maundy Thursday last year) and the fitness program I tried to implement. Mt. Apo is the Philippines’ highest peak (2,954 MASL) and also have one of the coldest open air temperature nigh time. Considered as a Level 3 (strenuous, major) climb, the “trip” to the peak consist 3-5 days of passing through wet, tropical rain forest, with some objective hazards, rope maneuvering, and walking for at least 6-8 hours a day on mostly steep slopes of up to 80 degrees. Mt. Apo is a popular destination for newbies and experienced climbers alike not only because of the bragging rights conquering the highest peak but also of the beauty that lies within that solemn mountain.
Here are my specific goals I set before I embarked climbing Mt. Apo last year:
- To be able to carry a 40 litre backpack (NF Flight Series) , for 6-8 hours a day, for 4-5 days.
- To be able to recover from climbing exhaustion for 8-12 hours sleep on a cold (0-5 degrees) night.
- To be able to ascent to the peak on summit assault day on usually 60-80 degrees slope and back.
My fitness program and physical conditioning starts well before the climb date usually at a minimum of one month. But effective training is noticeable after least 3 months, studies have shown. I usually go on interval climbs to train for another major climb though. And this might explain why I get conditioned even if my fitness program only start at least a month on some climbs. And the exercise I do are often, close simulation of climbing. Simulation and training climbs conducted by the author’s group, TAMAC, often on hills and benign trails like this one going to Lake Maughan in Tiboli South Cotabato is needed to augment climb conditioning
Simulation and training climbs conducted by the author’s group, TAMAC, often on hills and benign trails like this one going to Lake Maughan in Tiboli South Cotabato is needed to augment climb conditioningThe first few weeks is centered on getting myself into the routine of exercises, emphasizing discipline but at the same time, carefully observing myself for overenthusiasm injuries. Using a timed fitness program, I vary and progress my exercises depending on my month to month progress. It is usually a regimented but often flexible program that suits my work days and schedules.
There are many cardiovascular exercise you can do that may be available to you in your location. I chose exercises I can do easily in my place, like running, stairs climbing, biking or swimming. These exercises not only increases cardiovascular capacity, it also increases strength and endurance for climbing. Here are other benefits of cardiovascular exercise.
Some general guidelines for aerobic training:
- Aerobic training should be monitored by your heart rate or pulse rate, which should be 65%-80% of maximum heart rate. Maximum heart rate is computed by subtracting your age from 220. This should be your training heart rate.
- Training each day should be at least 30 minutes to one hour to be effective. A longer period of training time each day, on special locations and equipments is needed if your going for lengthier climbs.
- The frequency of training should be regimented but flexible. I train 2-3 times per week and daily near the climb date and watch myself for over use injuries. Rest is very much recommended between training weeks.
 When I developed discipline for training routines, I advance my cardiovascular training using interval training. Interval training includes upsurges in exercise intensity during an elevated heart rate and is very strenuous. Interval training when used over long period of times, increases the capacity of heart to pump blood even on emergencies and unexpected hazardous treks. Here are my examples.
When I developed discipline for training routines, I advance my cardiovascular training using interval training. Interval training includes upsurges in exercise intensity during an elevated heart rate and is very strenuous. Interval training when used over long period of times, increases the capacity of heart to pump blood even on emergencies and unexpected hazardous treks. Here are my examples.- On running, I start with a thirty minute moderate intensity pace then increase this pace 3 times for ten minutes then go back to moderate intensity. I repeat this every 20 minutes.
- Track or oval running includes running one round on moderate pace then sprinting 100 yards then one round again on moderate intensity.
 I use stretching, weights and calisthenics to develop my motor fitness. I have yet to develop an effective program with weights as I have at the moment very limited access to a fitness instructor, but I’m working on light weights (15kg) of 2 sets consisting of 20 reps each. Then I rest for 60 sec between sets. Stretching, calisthenics, abdominal and back strengthening exercises can be done daily.
I use stretching, weights and calisthenics to develop my motor fitness. I have yet to develop an effective program with weights as I have at the moment very limited access to a fitness instructor, but I’m working on light weights (15kg) of 2 sets consisting of 20 reps each. Then I rest for 60 sec between sets. Stretching, calisthenics, abdominal and back strengthening exercises can be done daily.
I also concentrate training on my lower extremity (thigh and leg muscles) and my upper torso, usually the back and stomach as this will help me carry my backpack. Strength motor training of upper and lower body should be done twice a week
Warming up and cooling down is an important part of my fitness program. I warm up 10 minutes before any exercise, with jogging or skipping ropes and bring my heart rate to my training range.
I do static stretching for 10-15 minutes before and after my fitness program workout. Stretching reduces muscular tension and prevents soreness after workouts and climbs. Any static stretching exercise should be held for 30 seconds.
Weight training should be focused on correct form and technique to develop the essential large muscles first, like the shoulder, triceps, biceps, quads and calf muscles. Leg curls, calf raises and squats strengthen the lower body and extremities while some exercises should be aimed in developing the chest, shoulders of the torso. For abdominal exercise, cross training the abdomen is beneficial. I highly suggest you seek advise from your fitness instructor regarding these strength training exercises and the correct techniques needed to do it.
I do one leg stand for my static balance exercise. This consist of standing on one leg holding the other leg’s foot then squatting and then returning to the standing one leg position. I do this two sets with 12 reps each.
I benefit much from badminton for my dynamic balance exercise, since I do this as a sport also. Aside from dynamic balance, I also gained some sort of cardiovascular strength from badminton, although this is just on the subjective point of view.
For most of my training regimens and physical conditioning, I try to keep a training record of my fitness program, more for discipline and assessing my improvements. I am certainly motivated and getting enthusiastic every time I see an improvement in my fitness status.
-
The Blog Rounds Second Edition; Internet and Philippine Medicine hosted by Prudence MD
The second edition of The Blog Rounds is up at Prudence MD. This week’s theme focuses on the impact of internet on medicine here in the Philippines. Read the whole edition here.
 (Cartoon grabbed from Prudence’s Blog)
(Cartoon grabbed from Prudence’s Blog)
The Blog Rounds is a weekly compilation of the best in Philippine’s medical blogosphere, written by physician bloggers (or the medically inclined blogger) and hosted on a participating physician blogger’s weblog.TBR archives and edition schedules are listed here. The next edition of TBR will be up next Tuesday 7am PST and will be hosted by Doc Cherry on Merry Cherry. Call for submission of articles will be announced by the host blogger soon.
Physicians and medically inclined bloggers interested in joining this blog carnival, please contact me through my email kokegulper[at]yahoo[dot]com or any of the participating TBR blogger. Guidelines and updates are posted here in my website, The Orthopedic Logbook.
-
Bone MD blogging back in The Orthopedic Logbook
After that scary Mt. Dulang-Dulang to Mt. Kitanglad traverse trek I joined 4 days ago (watch out for an upcoming post about this trek on my mountaineering blog, Talakudong Mountaineer at http://tacurongmountaineers.blogspot.com) , It’s nice to be back here, in the “comforts’ of my logbook. Dangling helplessly on those cliffs with just your bare hands holding on to a jutting tree root, I was praying I’m just blogging instead!
 The orthopod Bone MD on top of Mount Dulang-Dulang, the first stop of a 3 day D2-to K2 Traverse Climb he joined in Bukidnon
The orthopod Bone MD on top of Mount Dulang-Dulang, the first stop of a 3 day D2-to K2 Traverse Climb he joined in BukidnonBut I couldn’t resist this scenic view on top of Mt. Dulang. I hope this is worth the risks of the grueling traverse and the unfinished tasks I left here in TBR and Logbook.
-
The Blog Rounds First Ed at The Orthopedic Logbook : History of Medicine in the Philippines Made Ridiculous Hilarious!

“Before the diagnosis, there is diagnostics. Before the diagnostics, there is the physical examination. But before anything else, there is the history”.
This algorithm is the universally accepted and scientific method of diagnosing a disease in the medical world. One process may be concurrent with the other, but the whole algorithm is useless without knowledge of each one of these processes . More importantly to treat an ailment, you have to know the history of that ailment and the person afflicted with it.
History taking by far, is often a neglected part of this clinical evaluation process. Time constraints maybe, but sometimes, disasters could be avoided by just going back to the history of the patient.
In this week’s Blog Rounds, we go back in Philippine history, take a peek at some of the most interesting (often hilarious) health related trivia, diagnose a problem and offer some treatment pundits that mean something more than fill our stomach with gas while laughing about it. Our case?! Philippines medical history made ridiculously hilarious!

And keeping with the scientific rigidity we doctors hate to love, I, Bone MD, being the lucky moderator, will stick to that protocol and blog about it more hilarious than factual of course, but minus the edema and witch hunt! So throw off that white blazer, hang those stets, give that scalpel to your resident, grab some pizza, open those PCs, sit back and relax . Let’s fire off with the “cases” presented by our MD blogging colleagues!
Case No. 1: The Tragically Comic Cholera Epidemic of the Philippines
Blogger In Charge: Prudence MD History: The worst epidemic in the history of Philippines was said to be the 1902-1904 Cholera Epidemic. Worst, in all aspects. Read the full article by Prudence here.
History: The worst epidemic in the history of Philippines was said to be the 1902-1904 Cholera Epidemic. Worst, in all aspects. Read the full article by Prudence here.Physical Exam: Classic Cholera, yeah…by the hundreds of thousands of Filipinos! They’re dehydrating to death! Check their huts too and the dead bodies. (Their infected too?!!!)
Diagnostics: It’s the pooh Uncle Sam, bloody pooh in the Pasig River
Diagnosis: Cholera in epidemic proportions, from water source; but spread cannot be controlled expeditiously by our health authorities.
Treatment: Burn their huts, burn dead bodies , burn cholera with fire! Or throw them off Pasig River!!!Let’s infect fishes!
Comments: “If you don’t know whats killing your patient, might as well treat every possible diagnosis in your patient” Hence the “shotgun approach” of treating a disease. And yes if everything fails, burn them. Quite interesting though, this outbreak demystified the all knowing liberators we had before! Fire treatment?What gives?Case No. 2: Cause of Death
Blogger In Charge: Merry Cherry
History: Ever wondered how Philippine presidents die?Or why they died?More importantly, aren’t you interested why some presidents don’t die early when they’re supposed to?? Merry Cherry enumerates the cause of death of presidents , that might be of interest to the National Epidemiology Center of the Philippines, DOH, DOTC, Department of Agriculture and Philippine Congress (where pork is regulated, literally) and the Presidential Security Group. It may also interest the revolutionary strategist, the coup plotters and the TRAPOs aiming for the most powerful (and lucrative) seat in the land.
Physical Exam: I guess this is confidential, unless the president’s physicians share these data. Or if the PSG will allow us their charts. Part of EO 464 I believe
Diagnostics: You can ask all the Presidents and presidents- to-be to undergo stress tests, or stress 2D Echo. Pass a bill that will ban all politicians from taking any pork barrels and see which among them will have a heart attack. Ask for the services of an orthopod to open up any congressmen and see if their heart (if any) is fat laden. I believe some are harder than calcar. Don’t ask for PPD or sputum smear. If the president is negative, he is not Filipino.
Diagnosis: Dead Presidents; COD: As Described.
Treatment and Recommendations:If you’re into the political solutions for our health concern, take a look at how these presidents die. Perhaps our Department of Justice and health epidemiologists should not be worried. Cardiac and cerebrovascular disease ranks as the top two killers of presidents- not coup de etat, revolutions nor assassinations! These may have to be included in the security protocols of the PSG. No pork (barrels) for any congressmen or even for presidents!Case No. 3: The Filipina Doctor Coming in Full Circle
Blogger In Charge: Dr. ClaireBear: In the Middle of Nowhere
History: Dr. Clairebear narrates the colorful and often heroic women in medicine, from the Baybaylans of the pre hispanic era to the present modern day Filipina doctors standing equal or even better than their male colleagues.
Physical Exam: Gender differences not significant! The fact that the patriarchal society relegates them to the household and kitchen doesn’t mean they couldn’t and will not excel as healers.
Diagnosis: Filipina Doctors coming in full circle-Long, arduous battle against a patriarchal colonial system.
Comments: The babaylans– “seer, healer, community worker” of the pre-hispanic period were central to the healing of an ailing community. The role of women as healers in the Philippines has unfortunately been suppressed by the splurge of patriarchal colonizers of this country previously. The long and ardous battle is not against the opposite gender. It’s the pervading patriarchal colonial mentality that engulfs not only the medical world but also the entire nation.Case No. 4. P.D.A. (Public Display of Anesthesia)
Blogger In Charge: Doc Ness @Random Ness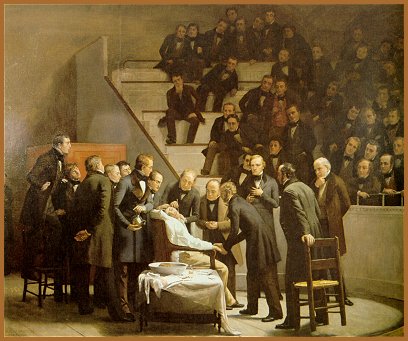
History: Doc Ness tells us the horrific history of anesthesia and how it came about silencing these howls. Or at least, tame them. The Filipino version of these “anesthetic” is virtually inexpensive and often mind boggling.
Physical Examination: Doc Ness, said, ” before, they die anyway. Why bother?”
Diagnostics: “Try a more volatile or a stronger gas. Let’s see who’s going to feel the pain while asleep” Try vocal anesthesia.
Impression: “If there is pain, gas him and hope he’d wake up after!”
Comments: While the howling success of PDA heralded painless surgeries worldwide, Philippines has our own brand of gas anesthetic, one that helps us survive the pains of living in an ailing healthcare system. No, not that gas pioneered in the chambers of the Nazi concentration camps. Jolly and ever humorous citizens of this country, we laugh-till-we-fart at the craziness of things going on around us, even if it slapped alarming trends in our health care system. Doc Ness calls it LA or “laway anesthesia” and believed this will ease pains of those who cannot afford the anesthetic even if the anesthesiologist is free! Or the words of politicians when they promise a treatment to a Juan in pain?Where did we get this trait? Cats and dogs lick their wounds to ease pain and heal it! I’m not sure this what Doc Ness is referring to.Case No. 5 : Sleep and Chocos
Blogger In Charge: Doc Hey: An eye doctor i the third world country
History: The classic story of unsung heroes in the medical field-less glamorous, often ill compensated physicians trying to cut their living while doing service to their countrymen. Doc Hey recants how she goes through her normal (20/20?) opthalmologic life, balancing her precious time with her family and the ever busy medical life.It graphically depicted some reasons for the continuing extinction of MDs in the provinces.
Physical Exam: May actually be a physical fitness feat rather than a physical exam. Or Sleep disorder in the making. For example, trying to sleep inside a car on your way to your son’s school. Doc Hey that early?Or maybe running around and racing stairways for OPD consults?
Diagnostics: Don’t ever try what Dr. Rizal (an opthalmologist) did as a diagnostic procedure in his time. He knew our country were run by rotten eggs at that time. He tried to prove this by being killed in Luneta.
Impression: Not all in history of Philippine medicine is misery. The fact is, most stories are heroic. Undaunted by the meager income and technological retrogression, the men and women of medicine survive each day with a smile on their face, seeing patients recovered and comforted. For Doc Hey even chocolates and cards are just bonuses.Summary of Findings: The history of medicine in the Philippines, is undoubtedly, one of the more interesting and sometimes annoying time
lines this world has ever witnessed. Dumb as some of this historical events maybe but we Filipinos laugh even in the worst of our lives. Our qualities as healers- empathy, kawang-gawa, meticulousness and loving care to name a few, remained the very reason why we are truly loved as healers in this world!Epilogue:
So, that’s all about this first edition of The Blog Rounds. I hope you find some interesting tidbits that painted smiles in your face.I would like to mention some contributors who submitted articles, but was not include in this edition because of technicalities in the guidelines. I will definitely forward your articles to future hosts when the theme is already apt for your articles.I call on the other blogger MDs (Bubbleman, Doc Ian, Pinay Megamom, Dak, Tetel) who promised to join TBR but have not submitted their posts yet, for one reason or another. Submit them. And for those who are interested to join, please do so and read the updates and guidelines in my blog The Orthopedic Logbook.
Due credits is also given to the owner of the pictures used in this posts!
The next T.B.R. will be up on Tuesday next week and will be hosted by Prudence MD.
Thank you all!











{kind=link}